Vertebral and carotid artery dissection: Difference between revisions
Neil.m.young (talk | contribs) (Text replacement - " w/ " to " with ") |
ClaireLewis (talk | contribs) |
||
| Line 13: | Line 13: | ||
==Clinical Features== | ==Clinical Features== | ||
===Internal Carotid Dissection=== | ===Internal Carotid Dissection=== | ||
*Unilateral | *Unilateral [[headache]], face pain, anterior [[neck pain]] | ||
**Pain can precede other symptoms by hours-days (median 4d) | **Pain can precede other symptoms by hours-days (median 4d) | ||
** | **Headache most commonly is frontotemporal; severity may mimic SAH or preexisting migraine | ||
*Partial Horner syndrome (miosis and ptosis) | *Partial Horner syndrome (miosis and ptosis) | ||
* | *[[Cranial nerve palsies]] | ||
===Vertebral Artery Dissection=== | ===Vertebral Artery Dissection=== | ||
*Posterior neck pain, HA | *Posterior neck pain, HA | ||
Revision as of 22:51, 14 July 2016
Background
- Most frequent cause of CVA in young and middle-aged patients (median age - 40yrs)
- Symptoms may be transient or persistent
- Consider in trauma patient who has neurologic deficits despite normal head CT
- Consider in patient with CVA + neck pain
Risk Factors
- Neck trauma (often minor)
- Coughing
- Connective tissue disease
- History of migraine
Clinical Features
Internal Carotid Dissection
- Unilateral headache, face pain, anterior neck pain
- Pain can precede other symptoms by hours-days (median 4d)
- Headache most commonly is frontotemporal; severity may mimic SAH or preexisting migraine
- Partial Horner syndrome (miosis and ptosis)
- Cranial nerve palsies
Vertebral Artery Dissection
- Posterior neck pain, HA
- May be unilateral or bilateral
- HA is typically occipital
- Unilateral facial paresthesia
- Dizziness
- Vertigo
- N/V
- Diplopia and other visual disturbances
- Ataxia
Differential Diagnosis
Neck Trauma
- Penetrating neck trauma
- Blunt neck trauma
- Cervical injury
- Neurogenic shock
- Spinal cord injury
Diagnosis
Denver screening criteria for blunt cerebrovascular injury
The Denver Screening Criteria are divided into risk factors and signs and symptoms
Signs and Symptoms
- Arterial hemorrhage
- Cervical bruit
- Expanding neck hematoma
- Focal neurologic deficit
- Neuro exam inconsistent with head CT
- Stroke on head CT
Stroke Syndromes
Anterior Circulation
Internal Carotid Artery
- Tonic gaze deviation towards lesion
- Global aphasia, dysgraphia, dyslexia, dyscalculia, disorientation (dominant lesion)
- Spatial or visual neglect (non-dominant lesion)
Anterior Cerebral Artery (ACA)
Signs and Symptoms:
- Contralateral sensory and motor symptoms in the lower extremity (sparing hands/face)
- Urinary and bowel incontinence
- Left sided lesion: akinetic mutism, transcortical motor aphasia
- Right sided lesion: Confusion, motor hemineglect
- Presence of primitive grasp and suck reflexes
- May manifest gait apraxia
Middle Cerebral Artery (MCA)

Patient with stroke (forehead sparing).
Signs and Symptoms:
- Hemiparesis, facial plegia, sensory loss contralateral to affected cortex
- Motor deficits found more commonly in face and upper extremity than lower extremity
- Dominant hemisphere involved: aphasia
- Wernicke's aphasia (receptive aphasia) -> patient unable to process sensory input and does not understand verbal communication
- Broca's aphasia (expressive aphasia) -> patient unable to communicate verbally, even though understanding may be intact
- Nondominant hemisphere involved: dysarthria (motor deficit of the mouth and speech muscles; understanding intact) w/o aphasia, inattention and neglect side opposite to infarct
- Contralateral homonymous hemianopsia
- Gaze preference toward side of infarct
- Agnosia (inability to recognize previously known subjects)
Posterior circulation
- Blood supply via the vertebral artery
- Branches include, AICA, Basilar artery, PCA and PICA
Signs and Symptoms:
- Crossed neuro deficits (i.e., ipsilateral CN deficits w/ contralateral motor weakness)
- Multiple, simultaneous complaints are the rule (including loss of consciousness, nausea/vomiting, alexia, visual agnosia)
- 5 Ds: Dizziness (Vertigo), Dysarthria, Dystaxia, Diplopia, Dysphagia
- Isolated events are not attributable to vertebral occlusive disease (e.g. isolated lightheadedness, vertigo, transient ALOC, drop attacks)
- Approximately 25% associated with aortic dissection
Basilar artery
Signs and Symptoms:
- Quadriplegia, coma, locked-in syndrome
- "Crossed signs" in which a patient has unilateral cranial nerve deficits but contralateral hemiparesis and hemisensory loss suggest brainstem infarction
- Sparing of vertical eye movements (CN III exits brainstem just above lesion)
- Thus, may also have miosis b/l
- One and a half syndrome (seen in a variety of brainstem infarctions)
- "Half" - INO (internuclear ophthalmoplegia) in one direction
- "One" - inability for conjugate gaze in other direction
- Convergence and vertical EOM intact
- Medial inferior pontine syndrome (paramedian basilar artery branch)
- Medial midpontine syndrome (paramedian midbasilar artery branch)
- Medial superior pontine syndrome (paramedian upper basilar artery branches)
Superior Cerebellar Artery (SCA)
- ~2% of all cerebral infarctions[1]
- May present with nonspecific symptoms - nausea/vomiting, dizziness, ataxia, nystagmus (more commonly horizontal)[2]
- Lateral superior pontine syndrome
- Ipsilateral ataxia, nausea/vomiting, nystagmus, Horner syndrome, conjugate gaze paresis
- Contralateral loss of pain/temperature in face/extremities/trunk, and loss of proprioception/vibration in LE > UE
Posterior Cerebral Artery (PCA)
Signs and Symptoms:
- Common after CPR, as occipital cortex is a watershed area
- Unilateral headache (most common presenting complaint)
- Visual field defects (contralateral homonymous hemianopsia, unilateral blindness)
- Visual agnosia - can't recognize objects
- Possible macular sparing if MCA unaffected
- Motor function is typically minimally affected
- Lateral midbrain syndrome (penetrating arteries from PCA)
- Medial midbrain syndrome (upper basilar and proximal PCA)
Anterior Inferior Cerebellar Artery (AICA)
- Lateral inferior pontine syndrome
- Ipsilateral facial paralysis, loss of corneal reflex (CN VII)
- Ipsilateral loss of pain/temperature (CN V)
- Nystagmus, nausea/vomiting, vertigo, ipsilateral hearing loss (CN VIII)
- Ipsilateral limb and gait ataxia
- Ipsilateral Horner syndrome
- Contralateral loss of pain/temperature in trunk and extremities (lateral spinothalamic)
Posterior Inferior Cerebellar Artery (PICA)
Signs and Symptoms:
- Lateral medullary/Wallenberg syndrome
- Ipsilateral cerebellar signs, ipsilateral loss of pain/temperature of face, ipsilateral Horner syndrome, ipsilateral dysphagia and hoarseness, dysarthria, vertigo/nystagmus
- Contralateral loss of pain/temp over body
- Also caused by vertebral artery occlusion (most cases)
Internal Capsule and Lacunar Infarcts
- May present with either lacunar c/l pure motor or c/l pure sensory (of face and body)[3]
- Pure c/l motor - posterior limb of internal capsule infarct
- Pure c/l sensory - thalamic infarct (Dejerine and Roussy syndrome)
- C/l motor plus sensory if large enough
- Clinically to cortical large ACA + MCA stroke - the following signs suggest cortical rather than internal capsule[4]:
- Gaze preference
- Visual field defects
- Aphasia (dominant lesion, MCA)
- Spatial neglect (non-dominant lesion)
- Others
- Ipsilateral ataxic hemiparesis, with legs worse than arms - posterior limb of internal capsule infarct
- Dysarthria/Clumsy Hand Syndrome - basilar pons or anterior limb of internal capsule infarct
Anterior Spinal Artery (ASA)
Superior ASA
- Medial medullary syndrome - displays alternating pattern of sidedness of symptoms below
- Contralateral arm/leg weakness and proprioception/vibration
- Tongue deviation towards lesion
Inferior ASA
- ASA syndrome
- Watershed area of hypoperfusion in T4-T8
- Bilateral pain/temp loss in trunk and extremities (spinothalamic)
- Bilateral weakness in trunk and extremities (corticospinal)
- Preservation of dorsal columns
Risk Factors
- Midface Fractures (Le Fort II or III)
- Basilar Skull Fracture with carotid canal involvement
- Diffuse axonal injury with GCS<6
- Cervical spine fracture
- Hanging with anoxic brain injury
- Seat belt abrasion or other soft tissue injury of the anterior neck resulting in significant swelling or altered mental status
If positive, CTA or MRA
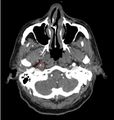
CTA brain showing filling defect in the R carotid artery (circled)

Management
Anti-coagulation followed by vascular repair is the generally accepted treatment. Anti-coagulation prevents clot propagation along the dissecting lumen[8]
tPA
- Do not give if dissection enters the skull (ie Intracranial)
- Do not give if aorta is involved
- Otherwise, give according to same guidelines as for ischemic CVA (see CVA (tPA))
Antiplatelet vs Anticoagulation Therapy
Very controversial with poor data
- Heparin: If dissection causes neuro deficits and is EXTRACRANIAL
- Aspirin: If dissection is INTRACRANIAL
- Aspirin: If dissection is extracranial but no neuro deficit, for prevention of thrombo-embolic event
- If tPA was given, wait 24hr before starting antiplatelet therapy
- Do not give if NIHSS score ≥ 15 (risk of hemorrhagic transformation)
Endovascular Therapy
- Emergent consultation with vascular surgery.
- tPA use does not exclude patients from endovascular therapy
Complications
- CVA
- Risk of stroke or recurrent stroke is highest in the first 24hr after dissection
- SAH (if dissection extends intracranially)
See Also
References
- ↑ Macdonell RA, Kalnins RM, Donnan GA. Cerebellar infarction: natural history, prognosis, and pathology. Stroke. 18 (5): 849-55.
- ↑ Lee H, Kim HA. Nystagmus in SCA territory cerebellar infarction: pattern and a possible mechanism. J Neurol Neurosurg Psychiatry. 2013 Apr;84(4):446-51.
- ↑ Rezaee A and Jones J et al. Lacunar stroke syndrome. Radiopaedia. http://radiopaedia.org/articles/lacunar-stroke-syndrome.
- ↑ Internal Capsule Stroke. Stanford Medicine Guide. http://stanfordmedicine25.stanford.edu/the25/ics.html
- ↑ DiPerna CA, Rowe VL, Terramani TT, et al. Clinical importance of the “seat belt sign” in blunt trauma to the neck. Am Surg. 2002;68:441–445
- ↑ Rozycki GS, Tremblay L, Feliciano DV, et al. A prospective study for the detection of vascular injury in adult and pediatric patients with cervicothoracic seat belt signs. J Trauma. 2002;52:618–623; discussion 623–624
- ↑ Sherbaf FG, Chen B, Pomeranz T, et al. Value of emergent neurovascular imaging for “Seat belt injury”: A multi-institutional study. American Journal of Neuroradiology. 2021;42(4):743-748
- ↑ Zinkstok SM, Vergouwen MD, Engelter ST, et al. Safety and functional outcome of thrombolysis in dissection-related ischemic stroke: a meta-analysis of individual patient data. Stroke. 2011;42:2515–2520.